A 27-year-old female with a six-month history of proteinuria close to the nephrotic range (2 +∼3+) and hematuria (2 +∼3+) was admitted to the clinic due to nephritic syndrome. She experienced transient gross hematuria six months ago, and subsequent reviews revealed persistent microscopic hematuria and proteinuria. There were no significant medical conditions in her past medical history. Upon admission, a physical examination showed bilateral mild pretibial edema, while other physical examination findings were normal.
Laboratory studies revealed the following findings: the complete blood count showed a leukocyte count of 6050/mm^3 with 50.2% neutrophils. The hematocrit was 35% with a hemoglobin level of 12.3 g/dL. Erythrocyte sedimentation rate (ESR) in the first hour was 42 mm. The C-reactive protein (CRP) level was 0.13 mg/L. Serum chemistry indicated a blood urea nitrogen level of 79.6 mg/dL, a serum creatinine level of 0.80 mg/dL, a low total serum protein level of 6.1 g/dL, an albumin level of 3.2 g/dL, and a total cholesterol level of 122 mg/dL. Furthermore, immunological tests showed a reduced serum IgG level of 774 mg/dL (normal range:860–1740 mg/dL), while the serum IgA, IgM, C3, and C4 levels were within normal range (239, 149, 97, and 23 mg/dL, respectively). Other serological tests yielded negative results for antinuclear antibodies, anti-double-stranded DNA antibodies, anti-neutrophil cytoplasmic antibody, anti-GBM antibodies, anti-Smith antibodies, and anti-phospholipase A2 antibodies. Serological markers for hepatitis B and C viruses were negative, as were serum tumor markers including carbohydrate antigen 19 − 9, alpha-fetoprotein, and carcinoembryonic antigen.
Urine analysis revealed hematuria (3+), proteinuria (2+), protein levels of 3230 mg/24 h, albuminuria levels of 2489 mg/24h, urine density of 1.013, and urine pH of 7. Abdominal ultrasound showed multiple small bilateral renal calculi without hydronephrosis and pyramidal echogenic foci consistent with MSK in both kidneys. Enhanced computed tomography (CT) scan showed increased diffuse density in the medullary area of both kidneys with small stones, leading to the diagnosis of MSK (Fig. 1).
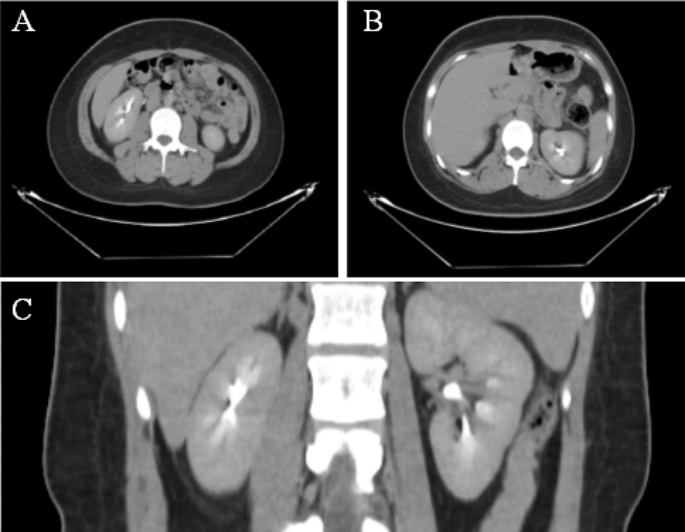
Enhancement CT of urinary system. Increased diffuse density in the medullary area of both kidneys with small stones. (A, B) Cross-section. (C) Coronal plane
A kidney needle biopsy was scheduled, given the proteinuria (3.23 g). Light microscopy revealed sclerosing lesions in 1 out of 10 glomeruli, with mild to moderate mesangial cell proliferation and moderate mesangial matrix expansion observed in some glomerular segments. Cellular crescent formation was present in 3 glomeruli, and fibrous crescent formation in 1 glomerulus. Renal tubules displayed localized atrophy, inflammatory cell infiltration in the interstitium, while the renal interstitial vessels appeared unremarkable. Immunofluorescent analysis showed diffuse IgA (2+) and C3 (+) staining across several mesangial areas (Fig. 2). The pathological diagnosis was focal segmental hyperplasia IgAN, according to the Oxford classification (M1E0S1T0C1). Electron microscopy examination showed there were more deposits of electron-dense material in the mesangial region of the glomerulus, the matrix in the mesangial region was mild to moderate increase increased, and partially foot process effacement of the podocyte (Fig. 3).
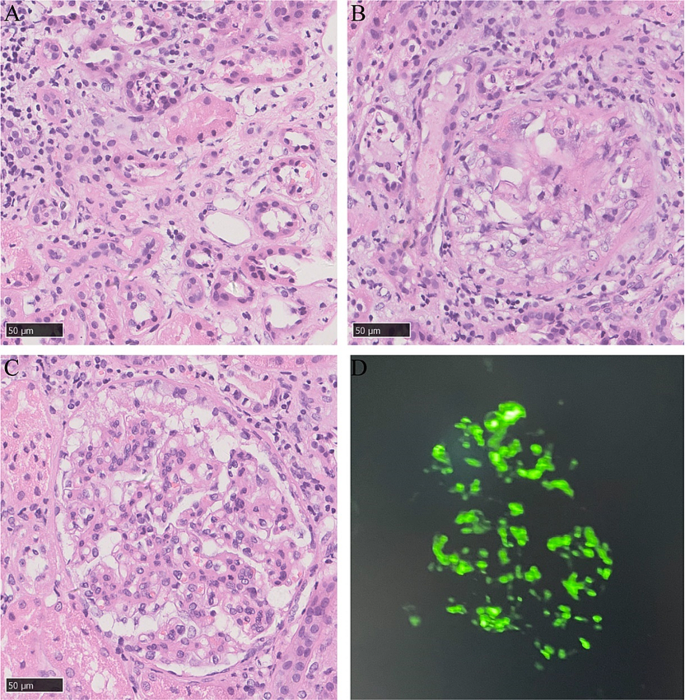
The light microscope results (A, B, C) and Immunofluorescent analysis results (D) of the patient. (A) Inflammatory cell infiltration in the interstitium(×400). (B) Cellular crescent formation was present in 1 glomeruli(×400). (C) Mesangial cell proliferation and mesangial matrix expansion (×400). (D) Diffuse IgA (2+) staining across several mesangial areas (×400)
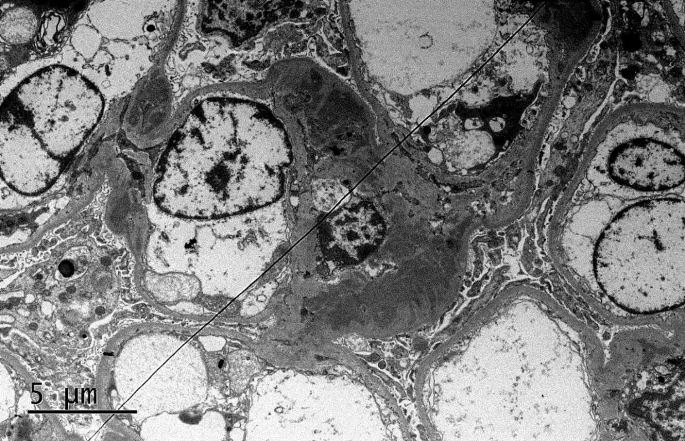
The electron microscope results of the patient. Electron-dense material in the mesangial region of the glomerulus and partially foot process effacement of the podocyte(×5,000)
We administered a combination therapy of oral prednisolone (40 mg qd, the subsequent dose was tapered) and losartan potassium Table (100 mg qd) to the patient. Following five months of treatment, the patient exhibited a partial remission of proteinuria and experienced relief from hematuria. The levels of serum albumin, serum creatinine, urine protein and urine erythrocyte of this patient on different dates are show in Table 1. The patient is currently undergoing treatment.
- The Renal Warrior Project. Join Now
- Source: https://bmcnephrol.biomedcentral.com/articles/10.1186/s12882-024-03596-w