Study population
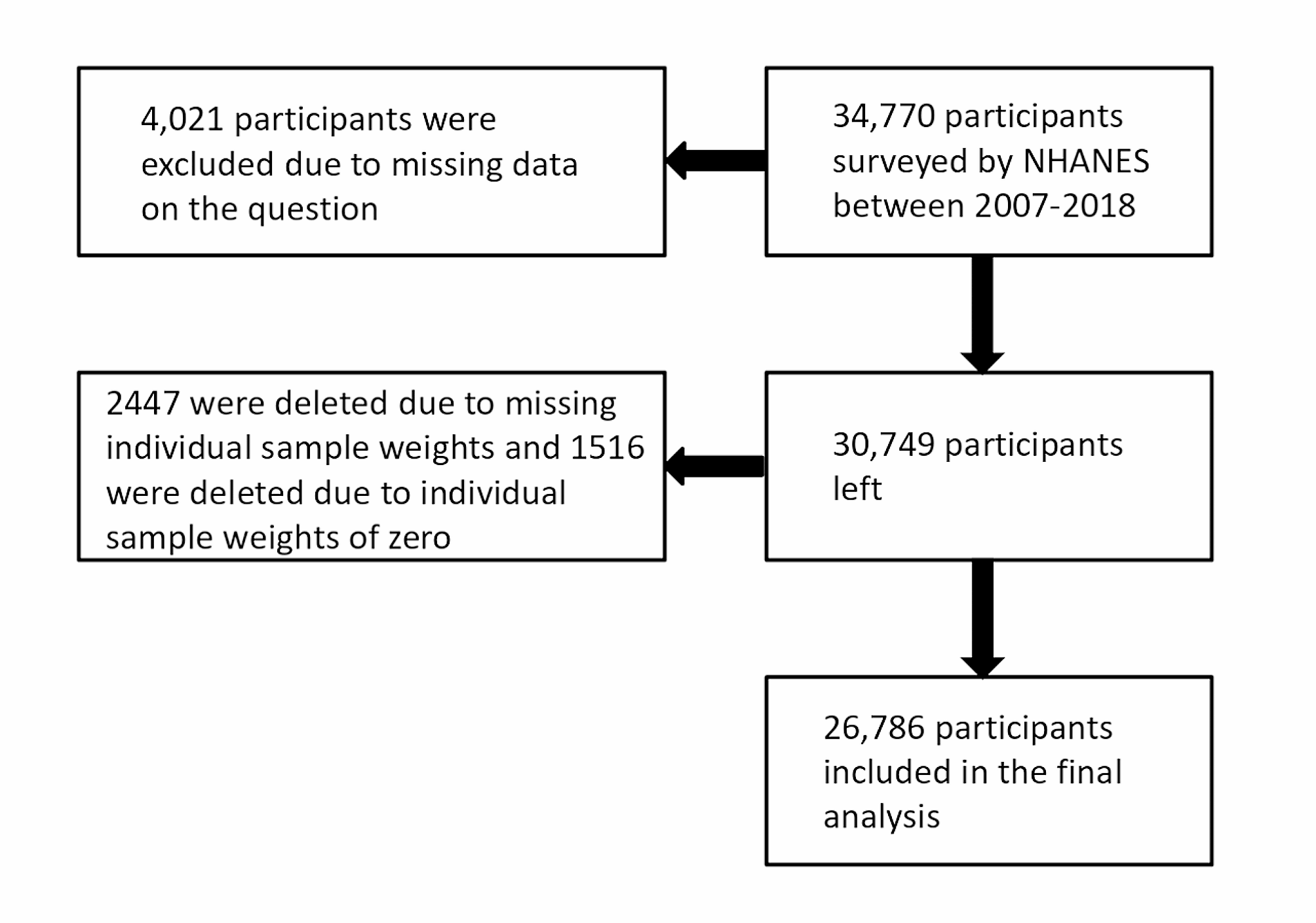
The National Center for Health Statistics (NCHS) annually surveys randomly selected, non-institutionalized U.S. civilians. Certain participant subgroups, such as the Hispanic, black, and elderly populations, are intentionally oversampled to reflect the U.S. population’s demographic composition accurately. The survey assessed the demographics, socioeconomic status, and health status of a nationally representative sample of U.S. residents. We analyzed respondents who completed relevant kidney status questionnaires over 6 NHANES cycles (2007–2018), including questions about kidney stones. Subjects who answered “refused,” “missing,” or “do not know” to questions assessing kidney stones were excluded. This study is a retrospective observational study.
Definition of kidney stones
Kidney stones were defined as an affirmative response to “Have you ever had kidney stones?” from a single survey question (KIQ026).
Oxidative balance score (OBS)
OBS was calculated based on a priori information on the relationship between O.S. and nutrients or lifestyle factors by screening 16 nutrients and 4 lifestyle factors, including 5 pro-oxidants and 15 antioxidants. Dietary intakes of 16 nutrients, including dietary fiber, carotenoids, riboflavin, niacin, vitamin B6, total folate, vitamin B12, vitamin C, vitamin E, calcium, magnesium, zinc, copper, selenium, total Dietary intakes of 16 nutrients, including total fat and iron, were obtained from the first dietary review interview.4 Lifestyle factors were physical activity, body mass index (BMI), alcohol consumption, and smoking, with the extent of smoking indicated by cotinine. Of these, total fat, iron, BMI, alcohol consumption, and smoking were considered pro-oxidants, and the rest were considered antioxidants. Referring to the method of calculating OBS, alcohol consumption was categorized into 3 groups, heavy drinkers (women ≥ 15 g / d, men ≥ 30 g / d), non-heavy drinkers (women 0 ∼ 15 g / d, men 0 ∼ 30 g / d), and non-drinkers, which were assigned scores of 0, 1, and 2, respectively. After that, the other components were grouped by gender and then divided into 3 groups by tertiles, where antioxidants were assigned a value of 0 ∼ 2, and pro-oxidants were assigned a value of 2 ∼ 0 in groups 1 ∼ 3 [12]. The higher the OBS scores, the more significant the antioxidant exposure. Subjects with ≥ 16 complete data for each of the 20 OBS components were selected for this study. For OBS with missing components, we assigned a score of 0 corresponding to the missing component, either antioxidant or pro-oxidant.
Assessment of covariates
In our study, covariates were certain factors previously shown or hypothesized to be associated with kidney stones or OBS, including sociodemographic variables, indicators of inflammation, diet quality, and comorbidities. Sociodemographic variables included age, sex (male, female), race (Mexican American, non-Hispanic black, non-Hispanic white, other Hispanic, other race – including multiracial), education (less than high school, high school, greater than high school), marital status (divorced/separated/widowed, married/living with a partner, never married), and the ratio of household income to poverty level (< 1.3, 1.3 ∼ 3.5, > 3.5). Inflammatory indicators reflected their status by the number of leukocytes, neutrophils, lymphocytes, and monocytes. Overall dietary quality was assessed using the 2015 version of the Healthy Eating Index (HEI) and total energy intake [13]. Comorbidities included hypertension, cardiovascular disease, diabetes mellitus, arthritis, and hyperlipidemia, with hypertension and diabetes mellitus diagnosed by index measurements, medication use, and self-report, and the remaining comorbidities identified by self-report.
Statistical analysis
All statistical analyses were performed using R version 4.3.0 (R Foundation for Statistical Computing, Vienna, Austria; http://www.r-project.org), and differences were considered statistically significant at a P value < 0.05. Weighting was performed using the NHANES-recommended weight selection and calculation method. Characterization of sociodemographic variables, inflammatory indicators, diet quality, comorbidities, and oxidative balance scores for the prevalence or absence of kidney stones was performed for the weighted data. In the baseline characterization, continuous variables were expressed as weighted means (standard errors), and categorical variables were expressed as sample sizes (weighted percentages). To test for differences in variable characteristics between OBS groups (quartiles), differences in weighted means for continuous variables were analyzed using ANOVA, and differences in weighted percentages for categorical variables were analyzed using the Rao – Scott χ 2 test to characterize the total population. A weighted logistic regression model explored the association between OBS and kidney stones. To validate the correlation between OBS and kidney stones and to explore the possibility of a nonlinear relationship between OBS and kidney stones, the continuous variable OBS was transformed into a categorical variable by quartiles, and a trend P value was calculated. A total of 4 models were used in this study, and the crude model did not adjust for any potential confounders. Model 1 adjusted for age, sex, race/ethnicity, marital status, poverty income ratio, and education. Model 2 further adjusted for white blood cells, neutrophils, lymphocytes, monocyte, Healthy Eating Index, and Total energy intake. Model 3 was additionally adjusted for five comorbidities. The OBS was categorized into dietary OBS and lifestyle OBS, and their associations with kidney stones were discussed separately. Finally, restricted cubic spline (RCS) regression was used to verify the relationship between kidney stones and OBS.
- The Renal Warrior Project. Join Now
- Source: https://bmcnephrol.biomedcentral.com/articles/10.1186/s12882-024-03607-w